BUILDING EXPERIENCED COHORTS
Before a fellowship year begins and fellows descend on Washington, D.C., a fellowship cohort must be built. The process and considerations for selecting fellows has evolved since 1973 but the ultimate goals has remained the same: identify outstanding mid-career health professionals with an interest in health and health policy.
The focus on mid-career professionals is key the Program’s ultimate goal to improve the health of the nation, a goal that has remained consistent across 50 years. Mid-career health professionals are experts in their field and can bring important insights into the policy making process during their placements. In addition, they tend to have both the experience and standing within their home institution to meaningfully apply what they learned in their year in D.C., whether that’s creating new courses on health policy to train the next generation, taking on leadership roles in their institution and/or state governments, or establishing new programs and centers with a focus on health policy work.
Mid-career professionals have the expertise to make a difference, and enough time left in their career to do the work.






From Health Care Policy to Health Policy
When the fellowship began in 1974, it was largely focused on health care policy: policy that affected patients and professionals in a clinical environment. Over the next few decades, as the health community began to realize that health is broader than health care and health care’s associated clinicians and nurses, so too did the program. Throughout its first 50 years, the RWJF Health Policy Fellowship has continually expanded its eligibility to better reflect society’s understanding of what and who determines the nation’s health.
“We began to recognize that health doesn’t just belong to health professionals. It belongs to so many other concerned and active leaders in this country that we opened our doors.”
— Marie Michnich, former Program Director and 1986-87 Fellow
Redefining Who Leads in Health
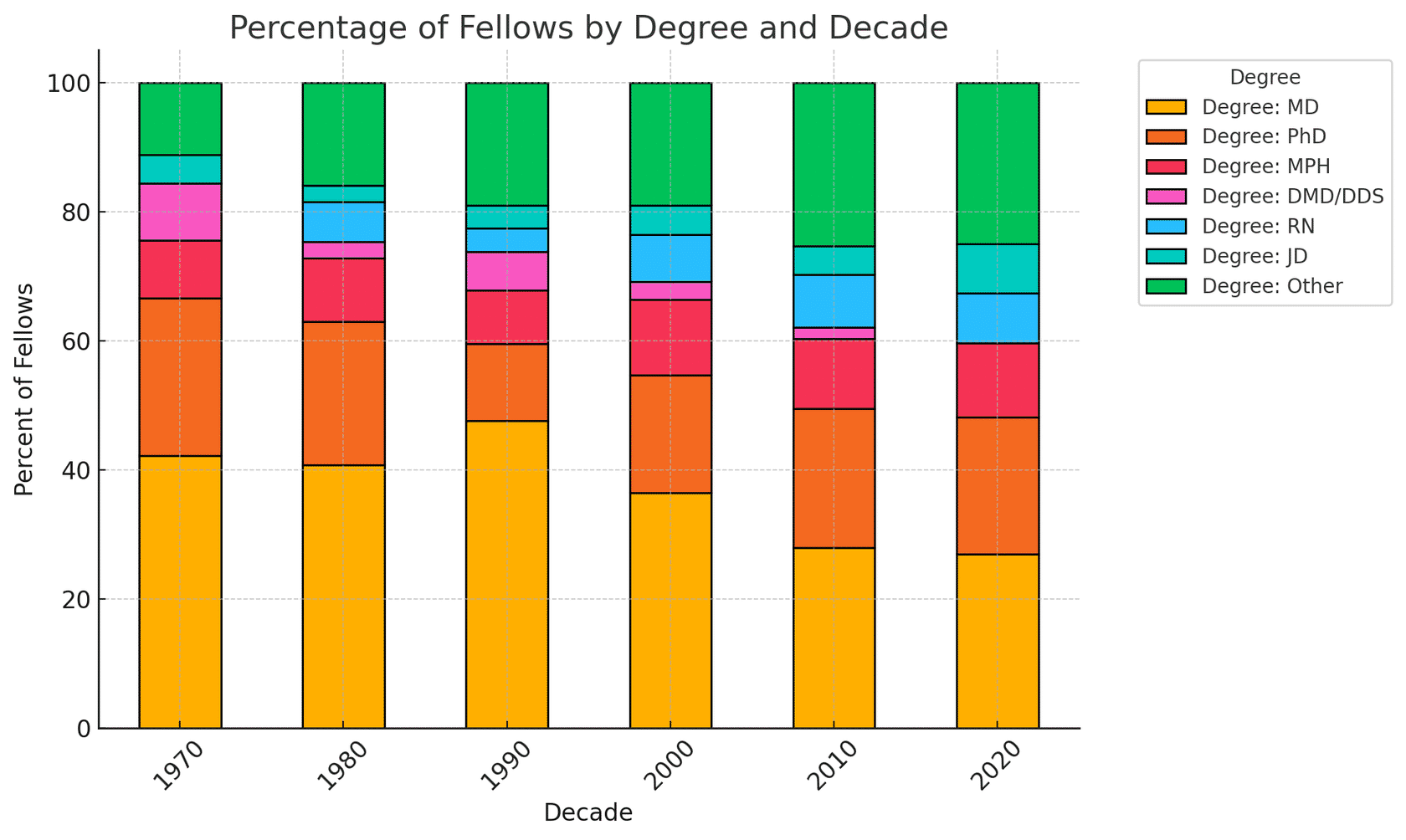
Since 1973, the Health Policy Fellowship has evolved its eligibility criteria for participants. Initially open only to academic medical faculty at select institutions, the program has gradually expanded to welcome professionals from economics, nonprofits, behavioral health, and government.
The timeline shows how eligibility criteria has expanded over five decades, reflecting a broader understanding of who shapes health in America.
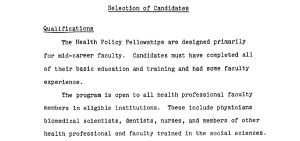
1973: Defining Eligibility in Academia
In 1973, eligibility for the Fellowship was limited to faculty from 114 academic health centers and institutions with medical schools. Applicants were nominated by the CEO of their institution, with only one candidate allowed per school. The process was intentionally selective, requiring letters, interviews, and a commitment from the institution to reintegrate the Fellow’s expertise after the program. This narrow scope focused on mid-career academic leaders and helped manage the program’s early scale. The Board noted that eligibility could be reconsidered if the program proved successful.
A 1973 Board memo outlined the original eligibility model, highlighting early selectivity and a narrow definition of who could shape health policy:
“The line obviously had to be drawn somewhere in accordance with definable and understandable criteria, and it was on this basis that the decision was made to set the parameters of the program in terms of academic health centers and other institutions with medical schools—a total of 114 institutions. It was considered highly probably that the mid-career academic faculty members who would most benefit from the fellowship experience would be found in this group of institutions.”
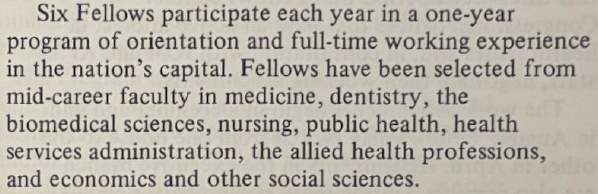
1975: Expanding to Include the Social Sciences
The 1975 program brochure shows the first expansion in eligibility to health professionals in the social sciences. Institutions were still allowed to submit only one nomination each, with the selection process remaining centralized through the Institute of Medicine.
View full 1975 program brochure.
1983: Welcoming Economists into Health
The 1983 brochure marked the first explicit inclusion of economics as an eligible field. Fellows continued to be drawn from mid-career academic faculty in health-related disciplines.
The 1983 brochure reflects the Fellowship’s acknowledgment that economic expertise is critical to national health policymaking.
 View full 1983 brochure.
View full 1983 brochure.
1994: Expanding Beyond Academia
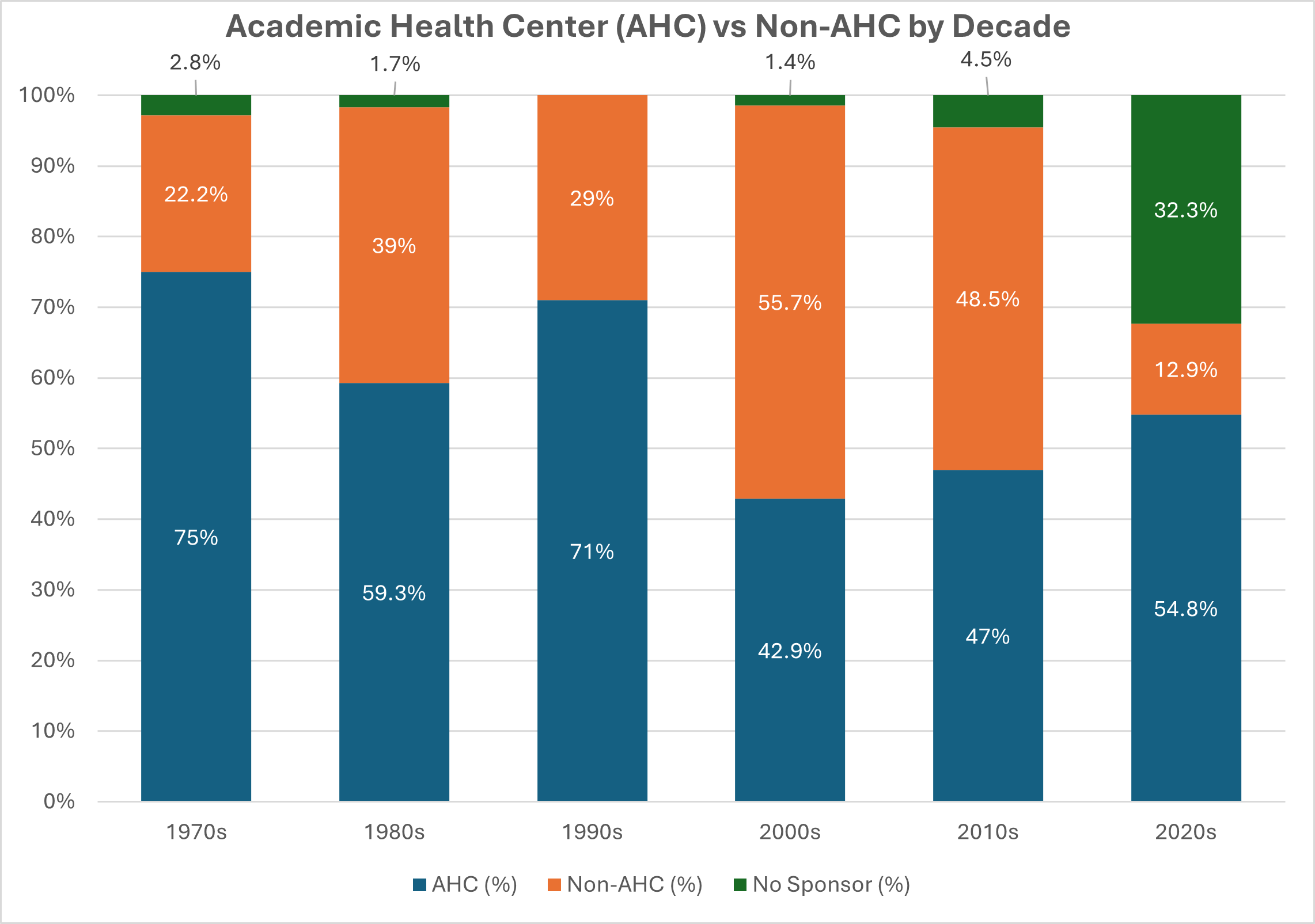
To better reflect the changing health marketplace, in 1994, the program expanded the institutions that could nominate a applicant from only academic health centers to include providers and institutions in the health care system, such as HMOs and related community-based organizations.
20??: Everyone Has a Stake in Health Policy
| The Fellowship has moved far beyond its original academic clinician roots. Today’s applicants come from public health, nonprofit leadership, government agencies, and academic institutions. Unlike earlier years, candidates now apply directly rather than being nominated by a sponsoring organization. | 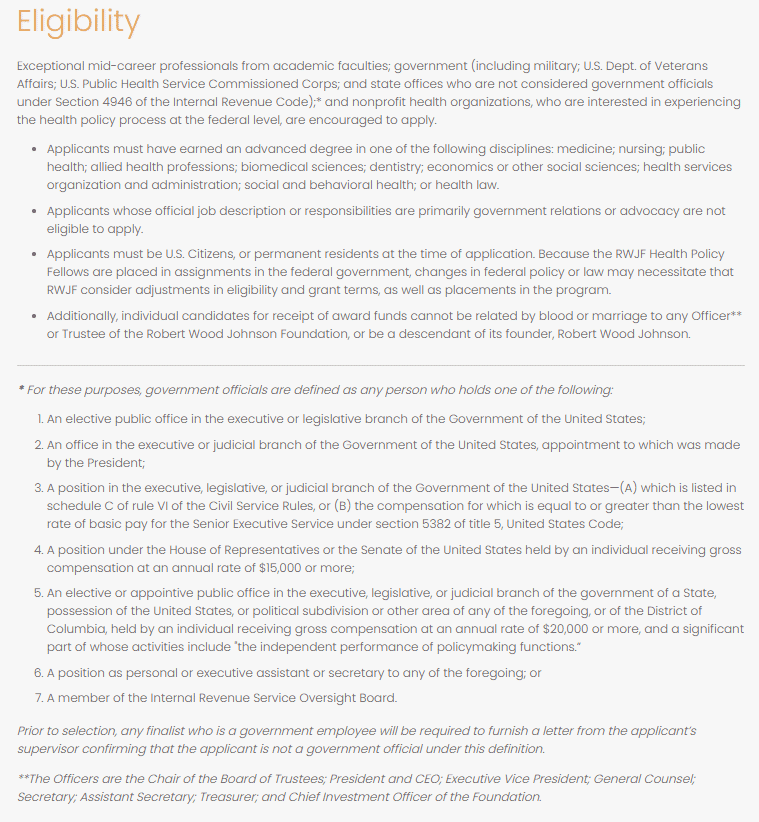 |
| Screenshot of the “Eligibility” page of the Health Policy Fellowship website, 2025. |
COMING TO WASHINGTON TO...
LEARN THE PROCESS
People apply to the RWJF Health Policy Fellowship Program from across the nation and with diverse backgrounds and disciplines, but accepted fellows all share the same underlying goal: to learn how health policy is made so that they can become more effective at improving the health of the nation.
GET PATIENTS THE CARE THEY NEED
CLOSE HEALTH EQUITY GAPS
BRING FEDERAL RESOURCES TO HOME COMMUNITY
IMPACT CHANGE ON A POPULATION LEVEL
CONNECT WITH THE PLAYERS IN HEALTH POLICY
BRIDGE RESEARCH AND POLICY
The Fellowship isn’t just a year in Washington;
it’s the start of a lifelong professional network.
Advisory Board members select cohorts with intention, and aim to balance geography, background, political views, and professional focus. The goal is not just to assemble impressive résumés, but to create a group that can challenge and learn from one another.
ADD TRANSITION TO NEXT SECTION (ORIENTATION)